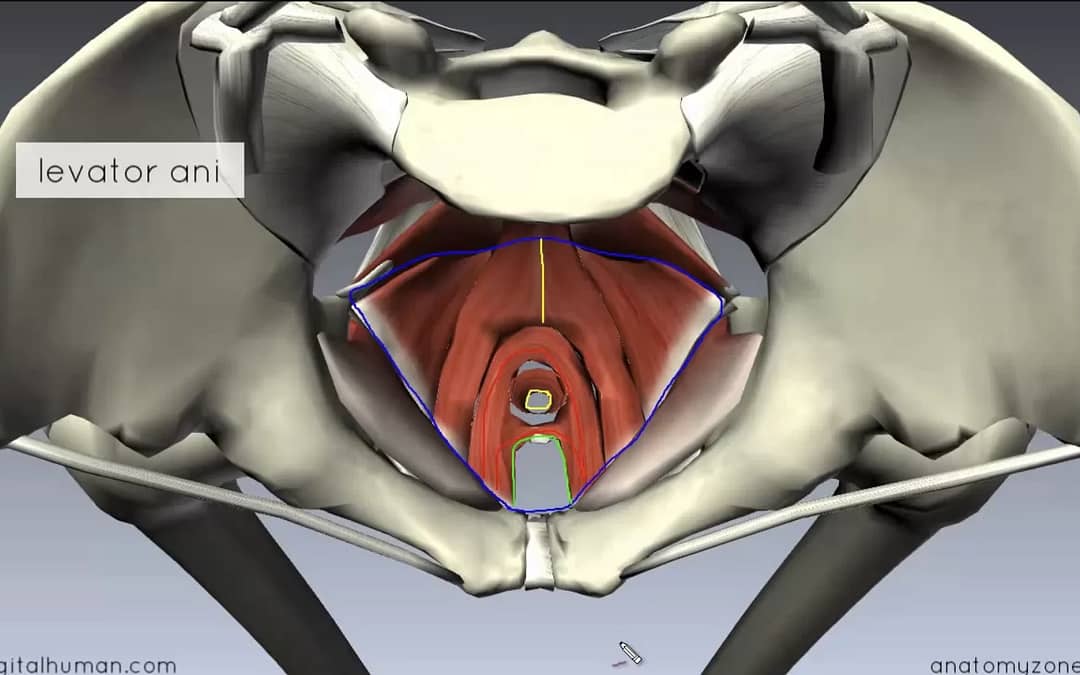
Low Back and Pelvic Girdle Pain – Understanding Pelvic Floor Connections
Understanding the connection between the pelvic girdle and the pelvic floor can improve low back pain and sacro-iliac joint patient outcomes. It can guide treatment, facilitate referrals, if needed, and improve patient quality of life.
Is the Pelvic Floor Balanced, Underachieving or Overachieving?
In my clinical practice, I regularly screened and evaluated my patients to determine the type of muscular dysfunction occurring in the pelvic floor. Overwhelmingly I would find overactive pelvic floor muscles in my patients with SI joint dysfunction and LBP. In cases like these, practitioners need to teach the patient to release the pelvic floor, rather than focusing solely on strengthening exercises. Understanding the connection between the pelvic girdle and the pelvic floor can improve patient outcomes.
What Does the Research Say?
In 2008, Eliasson, et al, found 79% of women with recurrent LBP experienced concurrent urinary incontinence (UI). This compares with 20-40% of the general population, depending on age. In 2016, Ghanderi, et al, built upon this research and showed that performing stabilization exercises with a focus on the pelvic floor led to improvement in both LBP and UI. Without the focus on the pelvic floor, LBP improved, but patients were still left with UI symptoms.
There is a growth in research supporting the connection between the pelvic floor, low back pain and pelvic girdle pain. New research shows this correlation goes beyond simple muscular weakness and points to a need to differentiate between patients with LBP who have pelvic floor muscle weakness versus an overactive pelvic floor. Ongoing research at McMaster University, School of Rehabilitation Science, in conjunction with Pelvic Health Solutions in Canada is helping to identify the incidence and type of pelvic floor dysfunctions associated with hip and LBP.
There is also a correlation between radicular symptoms and urinary incontinence. A 2016 study by Kaptan, et al, found a statistically significant correlation (p=0.001) between LBP with radicular symptoms and urge urinary incontinence. A relationship between stress urinary incontinence (SUI) was noted as well, however the correlation was not as strong. This was the first study specifically looking at radicular symptoms and UI, and more research is needed in this area.
Researchers have also looked at the incidence of pregnancy-related low back and pelvic pain (PLBP) and pelvic floor dysfunction. Pelvic floor dysfunction occurred in 52% of patients with PLBP, a significantly higher percentage than in the control group. These same women showed an increase in the muscular activity occurring in the pelvic floor muscles compared to healthy controls.
As a Physical Therapist, How Can You Help Your Patients?
First, recognize that many patients with low back pain, SI dysfunction or radiculopathy have pelvic floor complaints. To treat effectively and improve patient outcomes, addressing the pelvic floor component is necessary and beneficial. It is worth noting that unless specifically asked, many patients will not include urinary incontinence or pelvic pain in their initial complaints.
Second, learning to perform an external clothed exam can give a traditional orthopedic physical therapist a tool to assess pelvic floor muscle tone and strength. This allows integration of pelvic floor treatment, including stretch or release of overactive muscles, to help decrease pain and facilitate improved neuromuscular firing patterns. Providing postural education and breathing, and explaining how that affects the pelvic floor can also help.
Understanding the connection between the pelvic girdle and the pelvic floor can improve LBP and SI Joint patient outcomes. It can guide treatment, facilitate referrals if needed and improve quality of life.
Interested in Learning More?
If you are a pelvic health therapist interested in continuing education regarding pelvic health, please see Kathe’s Teaching page or consider hosting her (in person or virtually) for a course.
References
Eliasson, K., Elfving, B., Nordgren, B., & Mattsson, E. (2008). Urinary incontinence in women with low back pain. Manual therapy, 13(3), 206-212.
Ghaderi F, Mohammadi K, Amir sasan R, Niko kheslat S, Oskouei AE. (2016). Effects of Stabilization Exercises Focusing on Pelvic Floor Muscles on Low Back Pain and Urinary Incontinence in Women. Urology.;93:50-4.
Kaptan, H., Kulaksızoğlu, H., Kasımcan, Ö., & Seçkin, B. (2016). The Association between Urinary Incontinence and Low Back Pain and Radiculopathy in Women. Open Access Macedonian Journal of Medical Sciences, 4(4), 665–669. http://doi.org/10.3889/oamjms.2016.129
Personal communications Carolyn Vandyken, Nelly Faghani from Pelvic Health Solutions.
Pool-Goudzwaard, AL, Slieker ten Hove, MC, Vierhourt, ME, Mulder, PH, Pool, JJ, Snijders, CJ, Stoeckart, R.(2005). Relations Between Pregnancy-Related Low Back Pain, Pelvic Floor Activity and Pelvic Floor Dysfunction, Int Urogynecol J Pelvic Floor Dysfunct. Nov-Dec;16(6):468-74.
0 Comments